Criminalizing Abortion Kills.

Today Charles posted ‘One of the Most Disgusting Anti-Choice Articles You’ll Ever Read
Right wing man tries to deny the legacy of illegal abortion’
The right wing media are staging another one of their absurd freak-out sessions, this time pretending to be gravely offended by the use of wire coat hangers as a symbol of illegal abortion.
I grew up in Ireland, which up until last year, outlawed abortion under every circumstance. In 2013, Ireland reversed course somewhat:
In 2013, Ireland passed a new law allowing abortion under certain circumstances. On 30 July 2013, President Michael D. Higgins signed off on the Protection of Life During Pregnancy Act 2013 without referring it to the Supreme Court after meeting his advisers, the Council of State. The new law provides for a woman’s right to an abortion if her life is at risk, including from suicide
The reasons Ireland changed course on abortion is a long, dramatic, deadly story with real casualties, real harms, and real pain.
I’m going to examine some of those reasons here, but first, some facts about criminalizing abortion:
Every year, worldwide, about 42 million women with unintended pregnancies choose abortion, and nearly half of these procedures, 20 million, are unsafe. Some 68,000 women die of unsafe abortion annually, making it one of the leading causes of maternal mortality (13%). Of the women who survive unsafe abortion, 5 million will suffer long-term health complications. Unsafe abortion is thus a pressing issue. Both of the primary methods for preventing unsafe abortion—less restrictive abortion laws and greater contraceptive use—face social, religious, and political obstacles, particularly in developing nations, where most unsafe abortions (97%) occur. Even where these obstacles are overcome, women and health care providers need to be educated about contraception and the availability of legal and safe abortion, and women need better access to safe abortion and postabortion services. Otherwise, desperate women, facing the financial burdens and social stigma of unintended pregnancy and believing they have no other option, will continue to risk their lives by undergoing unsafe abortions.
(peer reviewed study in US National Library of Medicine National Institutes of Health)
According to the World Health Organization (WHO), every 8 minutes a woman in a developing nation will die of complications arising from an unsafe abortion. An unsafe abortion is defined as “a procedure for terminating an unintended pregnancy carried out either by persons lacking the necessary skills or in an environment that does not conform to minimal medical standards, or both.”1 The fifth United Nations Millennium Development Goal recommends a 75% reduction in maternal mortality by 2015. WHO deems unsafe abortion one of the easiest preventable causes of maternal mortality and a staggering public health issue.
From 1995 to 2003, the overall number of abortions declined, but the unsafe abortion rate was steady (from 15 to 14 abortions per 1000 women, respectively), constituting an increase from 44% to 48%.3
In Western nations, only 3% of abortions are unsafe, whereas in developing nations 55% are unsafe. The highest incidences of abortions that are unsafe occur in Latin America, Africa, and South East Asia (Figure 1).
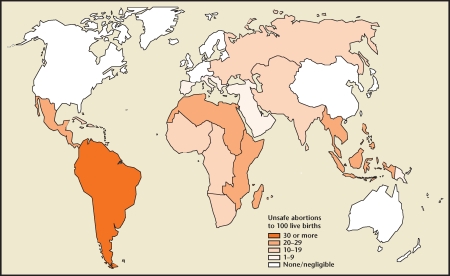 Unsafe abortion: global and regional estimates of incidence of unsafe abortion and associated mortality in 2003. via the World Health Organization.
Unsafe abortion: global and regional estimates of incidence of unsafe abortion and associated mortality in 2003. via the World Health Organization.Methods of unsafe abortion include drinking toxic fluids such as turpentine, bleach, or drinkable concoctions mixed with livestock manure. Other methods involve inflicting direct injury to the vagina or elsewhere—for example, inserting herbal preparations into the vagina or cervix; placing a foreign body such as a twig, coat hanger, or chicken bone into the uterus; or placing inappropriate medication into the vagina or rectum. Unskilled providers also improperly perform dilation and curettage in unhygienic settings, causing uterine perforations and infections. Methods of external injury are also used, such as jumping from the top of stairs or a roof, or inflicting blunt trauma to the abdomen.
Worldwide, some 5 million women are hospitalized each year for treatment of abortion-related complications such as hemorrhage and sepsis, and abortion-related deaths leave 220,000 children motherless.4,5 The main causes of death from unsafe abortion are hemorrhage, infection, sepsis, genital trauma, and necrotic bowel.1 Data on nonfatal long-term health complications are poor, but those documented include poor wound healing, infertility, consequences of internal organ injury (urinary and stool incontinence from vesicovaginal or rectovaginal fistulas), and bowel resections. Other unmeasurable consequences of unsafe abortion include loss of productivity and psychologic damage.
World abortion laws. Via the Center for Reproductive Rights.
The burden of unsafe abortion lies not only with the women and families, but also with the public health system. Every woman admitted for emergency postabortion care may require blood products, antibiotics, oxytocics, anesthesia, operating rooms, and surgical specialists. The financial and logistic impact of emergency care can overwhelm a health system and can prevent attention to be administered to other patients.
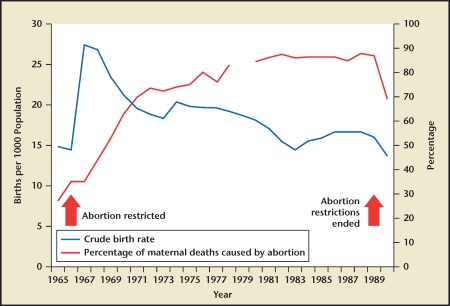 Live births and proportion of maternal deaths due to abortion. Reprinted from The Lancet, Vol. 368, Grimes DA et al, “Unsafe abortion: the preventable pandemic,” pp. 1908-1919, Copyright 2006, via Elsevier.4
Live births and proportion of maternal deaths due to abortion. Reprinted from The Lancet, Vol. 368, Grimes DA et al, “Unsafe abortion: the preventable pandemic,” pp. 1908-1919, Copyright 2006, via Elsevier.4The more access women receive to abortion and reproductive care the less likely they are to have abortions:
Less restrictive abortion laws do not appear to entail more abortions overall. The world’s lowest abortion rates are in Europe, where abortion is legal and widely available but contraceptive use is high; in Belgium, Germany, and the Netherlands, the rate is below 10 per 1000 women aged 15 to 44 years. In contrast, in Africa, Latin America, and the Caribbean, where abortion laws are the most restrictive and contraceptive use is lower, the rates range from the mid-20s to 39 per 1000 women.3
Less restrictive abortion laws also do not guarantee safe abortions for those in need; better education and access to health care are also required. In India, unsafe illegal abortions persist despite India’s passage of the Medical Termination of Pregnancy Act in the early 1970s. The act appeared to remove legal hindrances to terminating pregnancies in the underfunded (national) health care system, but women still turn to unqualified local providers for abortion. Clearly, the implications of the law never reached the population that most needed to rely on it.7 This example is also seen in Cambodia, where abortion is legally available on request and women often attempt to abort themselves before turning to hospital.8
The World Health Organization deems unsafe abortion one of the easiest preventable causes of maternal mortality.
Data suggest that even as the overall abortion rate has declined, the proportion of unsafe abortion is on the rise.
Methods of unsafe abortion include drinking toxic fluids; inflicting direct injury to the vagina, cervix, or rectum; or inflicting external injury to the abdomen. Complications also arise from unskilled providers causing uterine perforation and infections.
Worldwide, 5 million women are hospitalized each year for treatment of abortion-related complications, and abortion-related deaths leave 220,000 children motherless.
Data indicate an association between unsafe abortion and restrictive abortion laws.
Preventing unintended pregnancy, providing better access to health care, and liberalizing abortion laws to allow services to be openly provided can reduce the rate of abortion-related morbidity and mortality.
Abortion rates per region:
1. Western Europe
Countries: Austria, Belgium, Germany, Liechtenstein, France (pictured), Germany, Liechtenstein, Luxembourg, Monaco, Netherlands, Switzerland
Abortion rate: 12 per 1,000 women
2. Southern Africa
Countries: Botswana, Lesotho, Namibia, South Africa (pictured), Swaziland
Abortion rate: 15 per 1,000 women
3. Northern Europe
Countries: Aland Islands, Channel Islands, Denmark, Estonia, Faeroe Islands, Finland, Guernsey, Iceland, Ireland, Isle of Man, Jersey, Latvia, Lithuania, Norway, Sark, Svalbard and Jan Mayen Islands, Sweden, United Kingdom of Great Britain (pictured) and Northern Ireland
Abortion rate: 17 per 1,000 women
4. Oceania
Countries: Australia (pictured), New Zealand, Melanesia, Micronesia, Polynesia
Abortion rate: 17 per 1,000 women
5. Northern Africa
Countries: Algeria, Egypt, Libya, Morocco, South Sudan, Sudan, Tunisia, Western Sahara
Abortion rate: 18 per 1,000 women
6. Southern Europe
Countries: Albania, Andorra, Bosnia and Herzegovina, Croatia, Gibraltar, Greece (pictured), Holy See, Italy, Malta, Montenegro, Portugal, San Marino, Serbia, Slovenia, Spain, Yugoslav Republic of Macedonia
Abortion rate: 18 per 1,000 women
7. Northern America
Countries: Canada and the United States
Abortion rate: 19 per 1,000 women
8. South-central Asia
Countries: Afghanistan, Bangladesh, Bhutan, India (pictured), Iran, Maldives, Nepal, Pakistan, Sri Lanka, Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, Uzbekistan
Abortion rate: 26 per 1,000 women
9. Western Asia
Armenia, Azerbaijan, Bahrain, Cyprus, Georgia, Iraq, Israel (pictured), Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi Arabia, Syrian Arab Republic, Turkey, United Arab Emirates, Yemen
Abortion rate: 26 per 1,000 women
10. Western Africa
Countries: Benin, Burkina Faso, Cape Verde, Cote d’Ivoire, Gambia, Ghana, Guinea, Guinea-Bissau, Liberia, Mali, Mauritania, Niger, Nigeria, Saint Helena, Senegal (pictured), Sierra Leone, Togo
Abortion rate: 28 per 1,000 women
11. Eastern Asia
Countries: China (pictured), Hong Kong, Macao, Korea, Japan, Mongolia
Abortion rate: 28 per 1,000 women
12. Central America
Countries: Belize, Costa Rica, El Salvador, Guatemala, Honduras, Mexico (pictured), Nicaragua, Panama
Abortion rate: 29 per 1,000 women
13. South America
Countries: Argentina, Bolivia, Brazil (pictured), Chile, Colombia, Ecuador, Falkland Islands, French Guiana, Guyana, Paraguay, Peru, Suriname, Uruguay, Venezuela
Abortion rate: 32 per 1,000 women
14. Middle Africa
Countries: Angola, Cameroon, Central African Republic, Chad, Congo, Democratic Republic of the Congo, Equatorial Guinea, Gabon (pictured), Sao Tome and Principe.
Abortion rate: 36 per 1,000 women
15. Southeastern Asia
Countries: Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, Philippines, Singapore (pictured), Thailand, Timor-Leste, Vietnam
Abortion rate: 36 per 1,000 women
16. Eastern Africa
Countries: Burundi, Comoros, Djibouti, Eritrea, Ethiopia, Kenya, Madagascar, Malawi, Mauritius, Mayotte, Mozambique,
Abortion rate: 37 per 1,000 women
17. Caribbean
Countries: Anguilla, Antigua and Barbuda, Aruba, Bahamas, Barbados, Bonaire, Saint Eustatius, Saba, British Virgin Islands, Cayman Islands, Cuba, Curacao, Dominica, Dominican Republic, Grenada, Guadeloupe, Haiti, Jamaica, Martinique, Montserrat, Puerto Rico, Saint-Barth
Abortion rate: 38 per 1,000 women
18. Eastern Europe
Countries: Belarus, Bulgaria, Czech Republic (pictured), Hungary, Poland, Republic of Moldova, Romania, Russian Federation, Slovakia, Ukraine
This region has the highest abortion rate in the world, at 43 abortions per 1,000 women.
The new global abortion study - that’s published in the Jan. 19 issue of The Lancet - is from the U.S.-based Guttmacher Institute and the World Health Organization. Researchers found a link between higher abortion rates and regions with more restrictive legislation, such as in Latin America and Africa. They also found that 95 to 97 percent of abortions in those regions were unsafe.
These numbers are not lying - they clearly unequivocally show that criminalizing abortion endanger actual living humans lives. Women’s lives. Mothers lives.
Now back to the path to legal abortion in Ireland:
The story of abortion in ireland likely would not have changed in the last couple of years had it not been for the death of Savita Halappanavar.
Savita Halappanavar, a 31-year-old Indian native who was working in Ireland as a dentist, died at University Hospital Galway. She was suffering from a miscarriage when she was some 17 weeks pregnant on 21 October, 2012. She repeatedly asked for an abortion, however, she was told that, because Ireland was a “Catholic country,” she could not have one while the foetal heartbeat was still present, despite absolute medical opinion it was non-viable. The foetal remains were removed several days later on 24 October. Savita Halappanavar suffered septicemia and organ failure and died a few days later on 28 October 2012.
Ireland’s near-total ban on abortion has come under renewed scrutiny amid an outcry over the death of a woman who was denied a termination.
Savita Halappanavar, a 31-year-old dentist, died of blood poisoning at Galway University hospital. She had turned up at the hospital a week earlier, but was denied a medical termination and, according to her husband, was told: “This is a Catholic country.”The death intensified pressure on Ireland’s Fine Gael-Labour coalition to legislate and create specific guidelines for medical staff on when abortions can be carried out. At present, abortions are permitted only if there is a “real and substantive” threat to a woman’s life.
It was Savita’s suffering that brought change to Ireland - and while legalizing abortion was beginning to gain steam before her death - it is widely regarded that her death expanded the support for legal safe abortions, quite significantly.
A 1997 Irish Times/MRBI poll found that 18% believed that abortion should never be permitted, 77% believed that it should be allowed in certain circumstances (this was broken down into: 35% that one should be allowed in the event that the woman’s life is threatened; 14% if her health is at risk; 28% that “an abortion should be provided to those who need it”) and 5% were undecided.
A September 2004 Royal College of Surgeons survey for the Crisis Pregnancy Agency found that, in the under-45 age groups, 51% supported abortion on-demand, with 39% favouring the right to abortion in limited circumstances. Only 8% felt that abortion should not be permitted in any circumstances.
A September 2005 Irish Examiner/Lansdowne poll found that 36% believe abortion should be legalised while 47% do not.
A June 2007 TNS/MRBI poll found that 43% supported legal abortion if a woman believed it was in her best interest while 51% remained opposed. 82% favoured legalisation for cases when the woman’s life is in danger, 75% when the foetus cannot survive outside the womb, and 73% when the pregnancy has resulted from sexual abuse.
A January 2010 Irish Examiner/Red C online poll found that 60% of 18-35-year olds believe abortion should be legalised, and that 10% of this age group had been in a relationship where an abortion took place. The same survey also showed that 75% of women believed the morning-after pill should be an over-the-counter (OTC) drug, as opposed to a prescription drug.
A September 2012 Sunday Times/Behaviour and Attitudes poll of 923 people showed that 80% of voters would support a change to the law to allow abortion where the life of the woman was at risk, with 16% opposed and 4% undecided
.
A November 2012 Sunday Business Post/Red C poll of 1,003 adults showed that 85% of voters would like the government to “Legislate for the X case, which means allowing abortion where the mother’s life is threatened, including by suicide”, with 10% opposed and 5% undecided. The same poll also found that 82% of voters supported “A constitutional amendment to extend the right to abortion to all cases where the health of the mother is seriously threatened and also in cases of rape”, and 36% of voters supported “A constitutional amendment to allow for legal abortion in any case where a woman requests it”. In addition, 63% of voters also supported “A constitutional amendment to limit the X case, by excluding a threat of suicide as a grounds for abortion, but still allowing abortion, where the mother’s life is threatened outside of suicide”.
A January 2013 Paddy Power/Red C poll of 1,002 adults found that 29% of voters believed that there should be a constitutional amendment to allow abortion “in any case where the woman requests it”. 35% supported legislating for the X case allowing for abortions where the life of the mother is at risk, including from suicide. 26% supported legislating for the X case but excluding suicide and 8% believed no legislation at all was necessary.
A January 2013 Sunday Times/Behaviour and Attitudes poll of 916 voters found that 87% would support legislation to provide abortion where the woman’s life was in danger for reasons other than threat of suicide, 80% would support legislation to provide abortion where there was a foetal abnormality meaning the baby could not survive outside of the womb, 74% would support legislation to provide abortion where the pregnancy was a result of rape, and 59% would support legislation to provide abortion where the woman displayed suicidal feelings. Overall, 92% supported allowing abortion in one of these four circumstances, while 51% supported allowing abortion in all four circumstances.
A February 2013 Irish Times/Ipsos MRBI poll of 1,000 voters in face-to-face interviews in all constituencies found that 84% felt that abortion should be allowed when the woman’s life is at risk, 79% felt that abortion should be allowed whenever the foetus cannot survive outside the womb, 78% felt that abortion should be allowed in cases of rape or incest, 71% felt that abortion should be allowed where the woman is suicidal as a result of the pregnancy (the X case result), 70% felt that abortion should be allowed when the woman’s health is at risk, and 37% felt that abortion should be provided when a woman deems it to be in her best interest.
A June 2013 Irish Times/Ipsos MRBI poll of 1,000 voters in face-to-face interviews in all constituencies found that 75% were in favour of the government’s proposed legislation (the Protection of Life during Pregnancy Bill 2013), with 14% opposed and 11% choosing “Don’t know”. Furthermore, 89% felt that abortion should be allowed when the woman’s life is at risk, 83% felt that abortion should be allowed whenever the foetus cannot survive outside the womb, 81% felt that abortion should be allowed in cases of rape or abuse, 78% felt that abortion should be allowed when the woman’s health is at risk, 52% felt that abortion should be allowed where the woman is suicidal as a result of the pregnancy, and 39% felt that abortion should be provided when a woman deems it to be in her best interest.
Sources:
ncbi.nlm.nih.gov
ncbi.nlm.nih.gov
ncbi.nlm.nih.gov
ncbi.nlm.nih.gov
factcheck.org
un.org
irishtimes.com
irishtimes.com
thejournal.ie
rte.ie
businesspost.ie
rte.ie
en.wikipedia.org
rte.ie halappanavar
cbsnews.com
irishexaminer.com
en.wikipedia.org
en.wikipedia.org
irishexaminer.com
books.google.com
un.org
pila.ie
irishexaminer.com
merrionstreet.ie
independent.ie
abortioninireland.org
ncbi.nlm.nih.gov